
Turning Complexity into Success
Managing a High-Risk Calcified LAD with Perforation During PTCA
A 59-year-old patient with a history of PTCA to LAD and RCA (2007, 2016) was referred to our centre for CABG.
However, surgical revascularization was deferred due to a distally implanted LAD stent and an intramyocardial course of the vessel distal to the stent. The patient had a reduced ejection fraction of 35% with borderline hemodynamics, making the case particularly high risk.
The patient was therefore taken up for percutaneous coronary intervention (PTCA). Angiography revealed severe calcification, and a debulking strategy was planned using intravascular lithotripsy (IVL) ± cutting balloon.
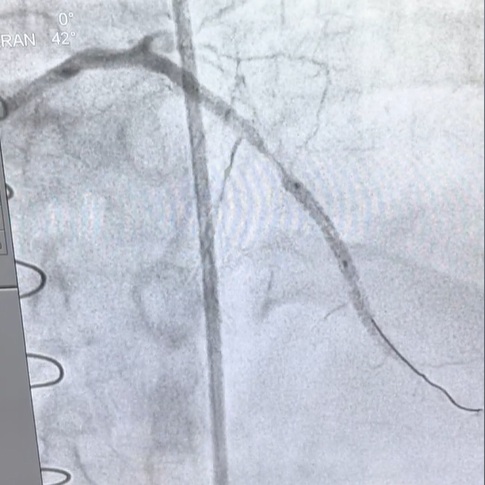
Predilation was initiated with a 2.0 mm balloon followed by a 2.5 mm balloon. However, this resulted in a serious complication—an Ellis Type III coronary perforation.
The patient was immediately managed with pericardiocentesis to stabilize hemodynamics. Given the complexity of the lesion and difficulty in delivering a Graftmaster stent due to an unprepared, heavily calcified ostioproximal segment, further lesion modification was required.
IVL (3 × 12 mm balloon) was used for debulking in the proximal and mid segments. However, guide extension catheters were unable to cross the ostioproximal calcific nodule. Additional lesion preparation was performed using an OPN NC 3 mm balloon.
Subsequently, an ostioproximal stent was deployed, which facilitated the successful passage of the Graftmaster stent across the perforation site. The perforation was successfully sealed.
Finally, a mid-LAD stent was deployed, followed by post-dilation. The final angiographic result was satisfactory, with restoration of vessel integrity and flow.
“`
